|
Honolulu Advertiser Second Opinion column by Cliff Slater February 18, 2002
|
|
|
Footnotes: (1) Personal communication with HMSA officials. For details, see table below. (2) Put another way, as a percentage of wages, the average Hawaii resident's health costs have more than doubled over the past eighteen years. See State Data Book, Table 12.27 for average wages. For health care costs, see U.S. Health Care Finance Administration On Line Statistics. 1998 State Estimates - All Payers - Personal Health Care. See chart and text below. (3) To a manufacturer, for example, health care costs are just another expense like taxes, payroll, or materials. If a manufacturers’ costs rise to the point where they can no longer compete with Mainland manufacturers than they will have to consider outsourcing, or moving, to the Mainland. (5) From the Towers-Perrin study: “More than 90% of the respondents reported that they expect double-digit increases to continue over the next few years. The survey indicates that the rising costs of prescription drugs is a primary reason behind the increase in health care costs.” “Technology As a Cause of Health Care Cost Growth: Many factors can lead to increases in health care costs above the rate of inflation. Demographic changes, the rapid spread of health insurance since the 1960s, and increased use of "defensive medicine" have all been blamed for rising health care costs. However, most analysts believe a large share of health care cost growth resulted from increases in the intensity of medical care caused by the introduction and rapid diffusion of new medical technologies (Fuchs, 1972; Warner, 1978; Goddeeris, 1984; Goddeeris and Weisbrod, 1985; Robinson and Luft, 1985; Luft et al., 1986; Schwartz, 1987; Noether, 1988; Weisbrod, 1991; Newhouse, 1993; Greenspan, 1998; Chernew et al., 1998). Fuchs (1996) found that 81 percent of health economists believe that a major share of rising health care costs can be attributed to increasing development, adoption, and use of new medical technologies.” (bold-face added). (6) See chart below. (7) From the study by Joanne Spetz and Laurence Baker. Has Managed Care Affected the Availability of Medical Technology? Public Policy Institute of California. May, 1999. “One driver of rapid technology diffusion is health insurance. People with health insurance demand more health care than is optimal because their insurance reduces their out-of-pocket expense below the true cost of health care. As individuals and physicians seek the most advanced medical care available, total health care expenditures rise, and these rising costs are billed to insurers. Because most Americans receive health insurance from their employers or the government, they are insulated from increases in the price of insurance that result from their preference for high-technology health care. Pharmaceutical and medical device firms continue to develop expensive technologies because they know that well-insured Americans will purchase their products with little attention to cost.” (8) The ASSOCIATION OF TRIAL LAWYERS OF AMERICA PAC is the eighth largest PAC in the nation. Review at Political Money Line. (10) House Progressive Caucus position on health care: 7. Institute Canadian-style single-payer health care reform. Provide health care to all Americans with no deductibles, no co-payments, no out-of-pocket expenses, and doctor choice. Insure that every person living in the U.S. receives quality health care regardless of race, gender, sexual orientation, income, age or ability. Author’s note: In time, a nationalized health plan may gain the consent of the electorate—but not the informed consent. As P.J. O’Rourke once warned about HillaryCare, “If you think health care is expensive now, wait until it’s free.” (11) Rationing care from limited funds. BBC News. January 11, 1999. “The NHS cannot, and never has been able to, offer every treatment to everyone who needs it.” UK moves towards national policy on NHS drugs. BBC News. September 15, 1998. “ … now health ministers accept that the plethora of costly modern medicines available put the NHS at risk, a spokesman said.” (13) MARTIN ZELDER. Canada no model for U.S. on health care. Scripps Howard News Service. May 22, 2000. |
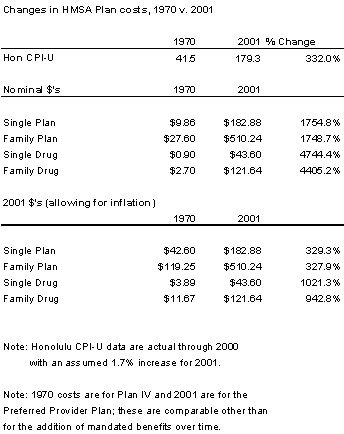
Health care soon unaffordable Private employers will need to either reduce employee working hours below 20 hours a week or lay off people and out-source their work offshore. Hawaii's current mandatory employer-based medical system is in danger of collapse in the long term because health costs are escalating far faster than payrolls and are becoming unaffordable for employers.. A little history: In 1970, premium HMSA family health coverage was $119 monthly with an additional $12 for drug benefits (in 2001 dollars allowing for inflation.) Today, the same family coverage has increased fourfold to $510 while drug coverage is up ten times to $122. (1) Soon they will double again. (2) Long before we get to that point, competitive pressures will force private employers to take other action since they have to at least cover their total labor costs. They will need to either reduce employee working hours below 20 hours a week (thus avoiding health care costs altogether) or layoff people and outsource their work offshore. (3) There have been and continue to be two main causes for these health cost increases. There is the increasing need for physicians to adopt costly defensive practices to protect themselves from potential lawsuits.(4) In addition, and most significantly, there has been the development and increasing use of newer and more expensive technology, especially drugs.(5) In order to keep health care costs down, employers have in the past ten years or so been switching to managed care (HMO's) and turning to other cost cutting measures. Health plan operators working under this employer-created pressure have been eliminating some high cost programs, increasing co-payments, squeezing doctors to discount their fees and, in general, shaving, scraping and manipulating wherever they can. However, much of this squeezing could only be a one-time affair and now health plan costs are rising again with double digit increases annually (see graph in footnotes). (6) What are the options? We can squeeze a little more from managed care—but not much. We can call a halt to continually bettering health care and settle for today's medical technology at today's prices—but that's hardly likely.(7) We could institute tort reforms—such as lawsuit losers paying court fees, outlawing contingency fees (as they are in most other countries), and capping liability awards. However, given the vast political contributions made by plaintiffs' attorneys, this is also not likely.(8) Failing these, we shall have no choice but to further manage (ration) health care. From the beginning of health plans in the 1930's and '40s all plans have formulated some denial of service in order to balance patients unlimited wants against limited financial resources. For example, limiting hospital stays and the use of expensive medical equipment, such as MRI's, or limiting expensive procedures such as transplants for older patients. When a lung transplant costs $250,000 with a 50/50 chance of surviving, an HMO manager is entitled to question whether it is a justifiable expenditure.(9) The nationalized health plans—euphemistically called single-payer plans—favored by Hawaii U.S. House members Abercrombie and Mink,(10) have even more extensive denials of service. For example, beta interferon for treating multiple sclerosis, Taxol for ovarian cancer patients and Viagra for impotence are denied to UK nationalized health care patients because they are so expensive.(11) And waiting lists for elective surgery in Canada and Britain can be years long.(12) That many Canadian and British citizens come to the U.S. for treatment testifies to the lower quality of nationalized health care in those countries. (13) With medical technology improving at an escalating rate, with costs rising accordingly, premium health care may, in time, no longer be affordable no matter what the delivery system. It is time that both our elected officials and our medical community address what is, on the face of it, a seemingly insurmountable problem. Cliff Slater is a regular columnist whose footnoted columns are at: www.lava.net/cslater Table for footnote (1)
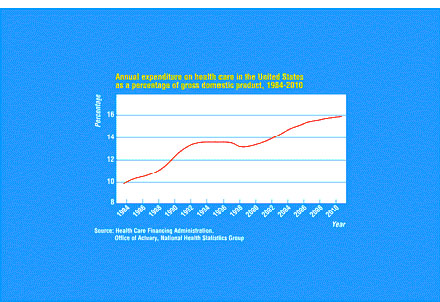
Graph with commentary for footnote (2)
Health care cost increases were contained in the 1990’s by wringing much of the excesses out of the health care system. Today, annual cost increases are back to climbing up in double digit percentages with no end in sight. From the Towers-Perrin study of rising U.S. health care costs: “For the second consecutive year, large employers will experience a double-digit increase in their health care costs, according to the recently released 2001 Towers Perrin Health Care Cost Survey. The annual survey found that the cost of large employers' health benefit plans will increase about 13% on average in 2001, the highest year-after-year percentage increase since Towers Perrin began conducting the survey more than a decade ago. Last year, Towers Perrin reported the average increase to be 12%.” |