|
Honolulu Advertiser Second Opinion column by Cliff Slater August 19, 2002 |
|
|
Footnotes: (1) See table below. (3) “The New Flu Drugs: Neuraminidase Inhibitors.” National Institute of Health. December 2000. (4) “Vanquishing a Virus: New drugs attack herpes infections.” Science News Online. April 13, 2002.
(5) “Lawmakers OK gas cap, prescription drug bills.” Advertiser, April 27, 2002.
(6) “Dems' long hold on Hawaii may be slipping “ USA TODAY; Aug 5, 2002; pg. A.04. Not online without fee.
(7) See Second Opinion, “Reducing Hawaii’s health care costs.” Honolulu Advertiser. July 22, 2002.
(8) “Pills, Profit and Public Health.” ABC News. May 30, 2002. |
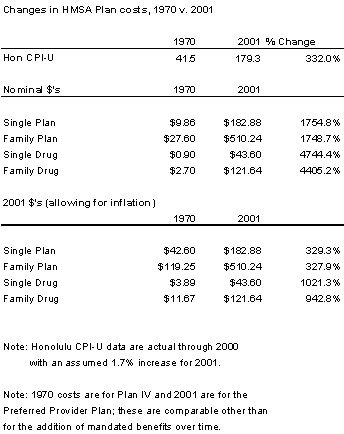
Hawaii’s drug costs need helpA recent column (2/18) discussed drug prices as the fastest-growing component of Hawaii’s burgeoning medical plan costs. Drug riders on HMSA family plans are now eleven times what they were in 1970 even after allowing for inflation.(1) In the old days, your doctor routinely prescribed “two aspirin and call me in the morning.” Now there are highly effective prescription drugs for nearly everything including migraine headaches,(2) influenza(3) and herpes,(4) all of which were not too long ago virtually untreatable; now they can be stopped. Even HIV deaths are down remarkably because of new drugs. Because of the Internet, physicians now have to deal with patients who are highly knowledgeable about their complaints even before their appointment. For example, when I needed malaria protection for a trip two years ago, I searched on the Internet and found that the U.S. Food and Drug Administration had just approved a new drug, Malarone, which had fewer side effects than the drug then in general use. Malarone had not been advertised and my doctor had not heard of it. I gave him my research and he prescribed it. It worked very well. Better information on drug availability through the Internet and TV advertising and, thus, the greater use of existing drugs has been one of the major causes of escalating costs. New drugs have contributed, but to a lesser extent. And it is a worldwide phenomenon—not just the U.S. What can we do about it? First, be grateful to the drug companies for developing these marvelous new drugs that allow us to live longer and better lives. They did not do it for us, of course. These greedy, rapacious lowlifes did it to fill their own coffers. We are just the beneficiaries—as long as we keep on paying enough for the drugs to fund the R&D. What can we do to reduce what we are spending on drugs? We can try the new Hawaii Rx program that will force manufacturers to negotiate drug prices with the state, which supporters believe will drive down prices 25 to 40%.(5) The concept of bureaucrats as hard-nosed in-your-face negotiators driving down costs seems somewhat strange. Their experience is in driving costs up. But let’s give it a try. And, while we are at it, if this plan works for drugs, why not food, clothing and shelter? And why stop there? This will be marvelous; we will no longer have to rely on the vagaries of the market. The Guardian State will just set prices for everything. No wonder that USA Today, describes us as, “one of the most centralized state governments in the nation.”(6) The trouble is that whenever governments have set prices in the past it has led to shortages. There was the Russian Loaf Syndrome where bread was cheap—but there wasn’t any. There were the gas lines of the 1970s. Or, simply, today’s downtown on street parking, which is also cheap, but there isn’t any. Another way is take the Medical Savings Account (MSA) approach. (7) Half the premium your employer pays goes to buy you a catastrophic health insurance plan covering any annual costs in excess of $2,000. The other half of the premium goes into a special account from which you pay your routine medical costs. What you don’t spend you keep in a tax-free IRA. This means that if you buy the $5 pill instead of the 50¢ one, you’ll have $4.50 per pill less in your MSA at the end of the year. It will make you think about the costs versus benefits. There are many instances of new drugs being as effective as the old ones but with some additional benefits or without certain side effects.(8) For example, as I recall, Malarone was ten times the price of the former leading anti-malarial drug yet they were both effective; the difference was fewer chances of side effects. Escalating drug costs in health care plans are here to stay—as are the benefits. And there is no free lunch. Cliff Slater is a regular columnist whose footnoted columns are at: www.lava.net/cslater Table for footnote (1)
|